From Major Diagnostic Category to All Patient Refined Diagnosis Related Groups
![[construction icon]](./images/worker.gif)
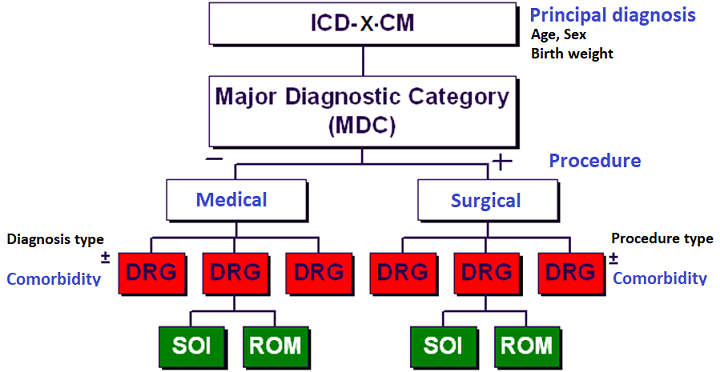
Hospital stays are being grouped into Major Diagnostic Categories (MDC) based on their primary diagnosis (ICD-x-CM). Subsequently each MDC is assigned to a Diagnosis Related Group (DRG) and an All Patient Refined Diagnosis Related Group (APR-DRG), which is homogeneous for medical treatment as for cost of treatment. A grouper software takes into account all the parameters and decides upon the MDC, DRG, SOI and ROM.
The Major Diagnostic Category is being used to calculate the average cost for each type of pathology and stay in the hospital to determine the acceptable activity (Dutch: verantwoorde activiteit). The acceptable activity is meant to match the activity within the hospital with its budget.
The Major Diagnostic Categories are being converted into All Patient Refined Diagnosis Related Groups (APR-DRG), which are more homogeneous for medical treatment as for cost of treatment. The classification of cure data into DRGs was for the first time developed at Yale University in the USA in the early 1970s. The purpose of a classification into DRGs is to relate the case mix of pathology of the hospital to its resource demand. Patients are being grouped into groups of patients with similar clinical profiles and demand of hospital resources (Resource intensity as the relative volume and types of diagnostic, therapeutic, and bed services used in the management of a particular disease).
The original goal for the development of the Diagnosis Related Groups (DRG) was to develop a system in which patients could be classified related to the hospital resources they consumed. However due to the evolution of healthcare, a new classification was needed which allowed for more than clasifying based on resource usage, cost and payment. A system was needed which would allow for more monitoring and control of medical activities, which became the APR-DRG classification:
The APR-DRGs expand the basic DRG structure by adding four subclasses to each DRG. The addition of the four subclasses addresses patient differences relating to Severity of Illness (SOI) (degree of physiologic decompensation or organ system loss of function) and Risk of Mortality (ROM, refers to the likelihood of dying). SOI and ROM indicate the requirement for the relative volume and types of diagnostic, therapeutic and bed services used in the management of a particular disease. The four Severity of Illness subclasses and the four Risk of Mortality subclasses are numbered sequentially from 1 to 4 ranging from minor, moderate, major, up to extreme Severity of Illness or Risk of Mortality. To evaluate resource use or to establish patient care guidelines, the APR-DRG in conjunction with severity of illness (SOI) subclass is used. For the evaluation of patient mortality the APR-DRG in conjunction with the risk of mortality (ROM) subclass is being used. The APR-DRG should lead to a more appropriate indication of the utilization of resources for the hospital and physicians, based on a more accurate severity-adjusted Case Mix Index (CMI).
The MDCs were created to ensure that the DRGs are clinically coherent. The diagnoses in each MDC corresponds to a single organ system or etiology and in general, MDCs are also associated with a particular medical specialty (medical, surgical). The basic organizing approach to classification in the APR-DRG system is to first assign the patient to a Major Diagnostic Category (MDC), based upon the principal diagnosis (PDX), and then to a specific APR-DRG category based upon principal diagnosis (if medical) or operating room (OR) procedure (if surgical). The principal diagnosis (PDX) is defined as the condition, after study, which occasioned the admission to the hospital. The principal diagnosis is not necessarily what brought the patient to the emergency room (ER), but rather, what occasioned the admission. A secondary diagnosis (SDX) is about comorbity (existed before admission, POA: Present On Admission) or a complication (occurred after admission). The principal procedure is the procedure most closely related to the principal diagnosis. A Secondary Proceure are all other significant procedures.
There are 25 Major Diagnostic Categories (MDC) defined:
In the APR-DRG system, the Severity of Illness (SOI) and Risk of Mortality (ROM) metrics are being used for illness and mortality risk adjustment within each Diagnosis Related Groups (DRG). The SOI indicates how sick the patient is, while the ROM indicates the likelihood of death of the patient. Besides SOI and ROM the system also takes into account the age and sex of a patient. In the APR-DRG system, a condition will impact a patient's SOI and/or ROM depending on what other conditions are present (comorbidities) along with their demographic information (age and sex). Each diagnosis has its own SOI/ROM value. A patient with a secondary diagnosis of uncomplicated diabetes mellitus type 1 (DM type 1) would have a Severity of Illness score of minor, or 1, while DM type 1 with ketoacidosis would be major, or 3. Be aware that the SOI and ROM are categories and not scores. The four levels of SOI and ROM are:

These webpages of course represent only personal interests, opinions and ideas and were created without a commercial goal. All views expressed on this site are my own and do not represent the opinions of any entity whatsoever with which I have been, am now, or will be affiliated. You may download, display, print and copy, any material at this website, in unaltered form only, for your personal use or for non-commercial use within your organization.
Should these webpages or portions of these webpages be used on any Internet or World Wide Web page or informational presentation, that a link back to this website (and where appropriate back to the source document) be established. Send a short notice by email when you copy these webpages, or part of it for your own use.
Any information here is provided in good faith but no warranty can be made for its accuracy. Although care has been taken in preparing the information contained in my webpages, I do not and cannot guarantee the accuracy thereof. Anyone using the information does so at their own risk and shall be deemed to indemnify me from any and all injury or damage arising from such use.
To the best of my knowledge, all graphics, text and other presentations not created by me on my webpages are in the public domain and freely available from various sources on the Internet or elsewhere and/or kindly provided by the owner.
If you notice something incorrect or have any questions, feel free to send me an email.
The author of this Webpage is Peter Van Osta
Email: pvosta at gmail dot com